


Why I Haven’t Died Yet: My Fifty Years with Diabetes
How I manage T1D while waiting for “the cure.”


Listen to this really fun AI-generated audio summary of this article.
On April 2, 1973, our family doctor informed us that I had type 1 diabetes (T1D), so I, a ten-year-old, would have to take daily insulin injections to stay alive. The good news, the doctors and others assured me with high confidence, was that a cure was only five to ten years away! All I had to do was, well, wait. And stay alive by taking insulin.
Many other T1Ds have heard similar claims when they were diagnosed–even to this day–which contributes to the running joke within the community, “The cure for diabetes is only five or ten years away… and always will be.”
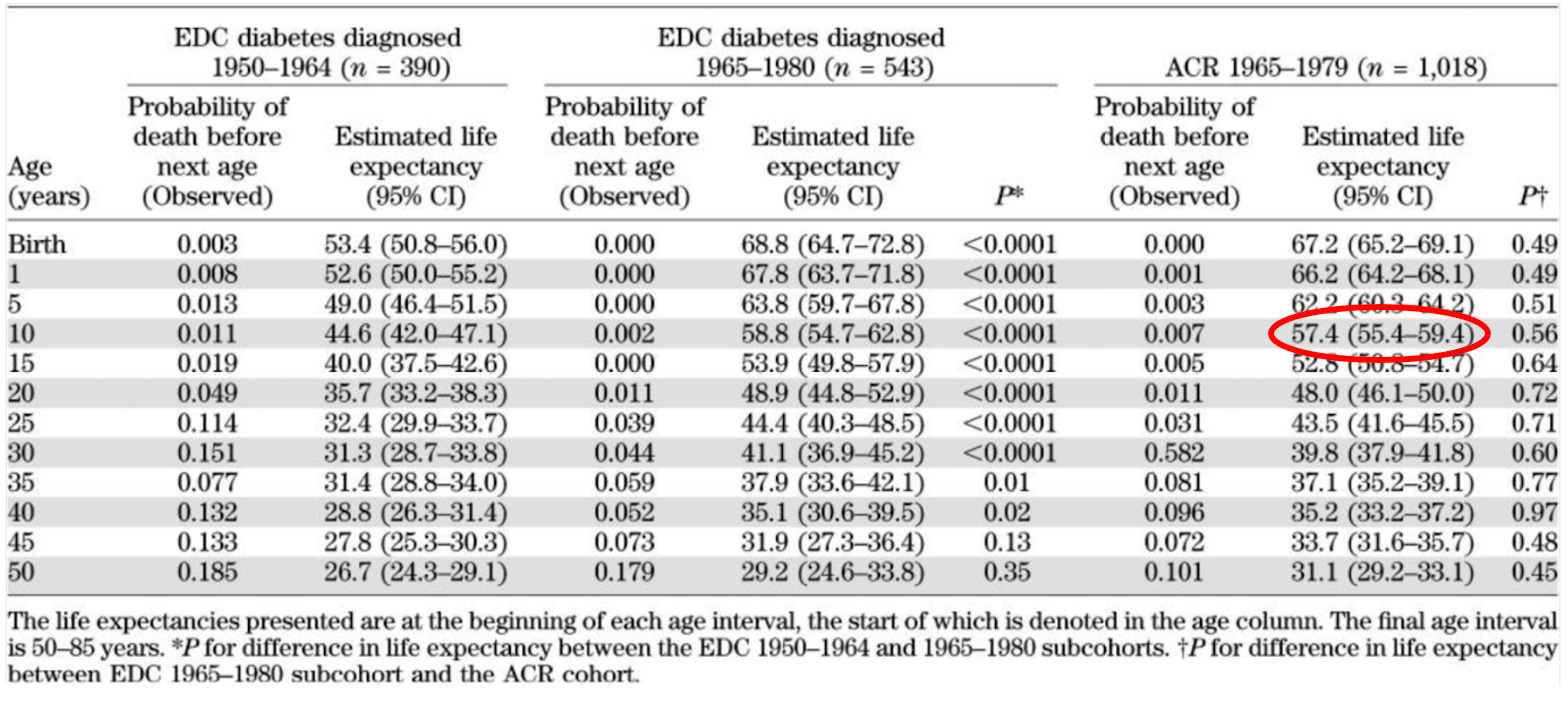
Despite the fact that we’re still waiting for that elusive cure, I managed to live longer than I was supposed to. A literature review of studies that estimate the life expectancy of T1D estimated that I would live to 57.4 years. (I joke that my birth certificate actually has an expiration date.)
Yes, here in 2023, I’m still alive at 60. Or, so I think. But, how do we really know? As you ponder that, here are a few fun stats about my fifty years as of April 2, 2023:
Total number of days living with T1D: 18,262
Number of insulin injections: 146,100 (average 8 per day)
Total amount of insulin taken: 1.74 gallons (~36 units per day over 50 years: 657,432 units)
Total blood glucose meter tests: 109,575 (1990-2020 / 10 strips/day)
Longest consecutive hours TIR (time-in-range): 207 (8.625 days)
Carbs/day: 426g (40% carbs, 30% fat, 20% protein)
Exercise: 147 mins/day (10.8mi/day – running/walking/hiking)
Highest and Lowest A1c: 7.8% and 5.5%, but I recall >8% in the mid-1980s
This may look impressive, but looks can be deceiving. My first 45 years of living with T1D were far from spectacular. Actually, it was because of my poor health that I figured I should probably manage the disease better, especially since it looked like a cure is still another five or ten years away.
No, seriously! In the 1990s when I was in my 40s, they were tinkering with islet cell implants that would be the norm for curing diabetes. When would it be available? Wait for it—about five years. Same with artificial pancreases: An automated insulin pump was going to relieve all self-management requirements by, wait for it, 2001!
Fast-forward to 2018, when my blood pressure started to elevate, my cholesterol levels were too high, and I was worried that the “enjoy by” date on my birth certificate was nearing its end.
My health recovery process began by getting a Dexcom G6 in 2018, which allowed me to track glucose levels. Immediately, I saw positive results. The chart below shows my A1c levels from 2001 to April 2023.

Yes, the CGM helped me fine-tune my dosing and carb protocol such that my A1c dropped from 7.3% to 6.5% in three months. My doc gave me a shiny gold star sticker and a sugarless lollipop, and told me that these stats were really good, and that I really shouldn’t try to do better. (My insurance wouldn’t cover the lollipop, so I had to give it back, or pay $8 for the out-of-pocket charge.)
This isn’t the first time I heard that an A1c of 6.5% was good, nor was it the first time I achieved it. I actually did it once before, in 1985, but I’ll get to that later.
Back to 2018: When I got my CGM and was able to see how insulin behaved relative to carbs and exercise, I learned a lot but was still having way too many hypo events: I’d get nightly readings <70 mg/dL, and many times <50 mg/dL, often waking up in a cold sweat.
No wonder my A1c was so low—it looked good on paper, but the unhealthy lows were devastating. (This is why I get upset with marketing materials that say, “lower your A1c!”, when instead they should say, “Improve your A1c.” There are a lot of T1Ds who are obsessed with high A1c levels and overdo their insulin intake.)
The real problem was that it was too hard to incorporate exercise into my daily regimen. Keep in mind, when my A1c’s were in the 7s, I could exercise extensively because I had far too much glucose onboard all the time. Hypos were rarely a concern. (In fact, if it weren’t for the exercise, my A1c’s would have likely been in the 8s or 9s.)
So, in an effort to learn how to reduce my hypo events, while also exercising, while also staying in range as much as possible, I went beyond my normal health care team and started my real journey: reading medical literature specifically on the human metabolic system. And wow, was I surprised: Not only is the natural human body far more complicated than most people are aware of, but T1D itself is insanely complex. I don’t think even most endos are even aware of the subtler nuances of how glucose is metabolised by the mitochondria. For example, ask your endo about the “lactate shuttle…” Yeah, lactate is a big deal, especially for T1Ds that exercise, and no one ever talks about it.
But here’s the kicker: What I learned from all this medical literature, while interesting, merely reinforced the four basic rules of T1D management: Watch your CGM to recognize your glycemic patterns, make small adjustments throughout the day (with insulin and carbs as needed), log your activities (food, exercise, insulin) and exercise. Yes, those four things are all you need to know…and do.
For a deeper dive into these four habits, which also explains how it’s much easier to do than you might think, see my article, “Self-Identity and the Four Habits of Healthy T1Ds.” One of the key points about these habits is that, if you adopt them, you don’t need “goals” or “targets” as those can be distracting at best, and dispiriting at worst, either of which can defocus your attention from the habits.
By focusing solely on processes, not goals, my A1c dropped to 5.5 - 5.8%, and my time in range (70-180) to 95%, with less than 1% of time below 70 mg/dL, and about 4% time above 180 mg/dL. This is on par with very healthy non-diabetic people.
Let me reiterate: These are not goals. I wasn’t trying for that. I simply refocused my attention on the four basic habits. And it was then that I also remembered back in that hospital room in 1973 when I was told I was a diabetic: My doctor told me to follow four basic tasks: Test urine for glucose “spillage” (even though the results were entirely useless), write down food and insulin (even though no one looked at it), and take insulin at least four times a day—one dose of long-acting insulin, and then three shots for each meal. How much? Hell, who knows! Trial and error. Oh, and try to exercise.
Believe it or not, I sorta, kinda, tried to do those things off and on over the next 45 years, and looking back, what it really did was teach me to remain engaged with diabetes. Not to fear it, get angry about it, or go into denial. It just was part of who I am.
Turned out, watching my CGM isn’t hard. Bolusing insulin for meals isn’t hard. Nothing is technically difficult. Keeping that in mind shifts the notion of managing T1D from “hard” to, well, “curious.”
There was another big influence in my life: an old girlfriend I had in 1985 who was deaf. She challenged me by asking, “Are you a diabetic, or a person with diabetes? Because to me, you act like the latter: Someone that doesn’t want to take care of themselves.” You can read about it in my article, The Sound of Diabetes.
Notice that I did not mention diets, or whether I use an insulin pen or a pump. Ok, fine. I use an insulin pen, but that doesn’t matter, because good glycemic control requires paying attention to your glucose levels, and taking actions when necessary. And you can do that with either a pen or a pump, but there are other considerations as well. For more on this, see “Benefits and Risks of Insulin Pumps and Closed-Loop Delivery Systems.”
Oh, one more thing: Managing T1D is an art, not a science. You have to know yourself and how your own body works. T1D is highly personalized because everyone’s metabolic system is different. It cannot be reduced to an algorithm. True, many believe that we will have AI-powered automated insulin delivery (AID) systems do all this work for you within the next five years. And they may be right, because I’ve been hearing about that since the 1990s. If you’re curious what they’re up against, read my analysis in my article, The Insulin Absorption Roller Coaster and What You Can Do.
Lastly, it might seem a bit trite and sappy to say, but having a long-term vision for yourself is key. This is where psychologist Brian Little’s concept of “free traits” comes in. Here, he’s referring to traits that may include certain proclivities, such as introversion, or attraction to risks, or predisposition to sweets, but they are “free” in that they can be curtailed when something is important to you — a “core project.”
My “core project” is my desire to one day pick up future grandchildren. I don’t want to blandly stare at them from a hospital bed with tubes keeping me alive as drool drips from the corner of my mouth, all because I didn’t take care of myself when I was younger. What an awful future that would be. I want to remain very healthy, just as I am right now, and be ready for when those grandchildren come screaming into my house yelling, “Grampa!”
I know it’ll happen too, because my son continues to promise me that future grandchildren is only five years away!
To learn more about current attempts to cure T1D, see my article, What a “Cure” for Diabetes Might Look Like.
HI Dan, I've read this article several times and have shared it with the education staff at my son's pediatric endocrinologist office. My son has been using the G6 since we switched back from the G7 in March after 3 months of impacted TIR. My concern now is what will happen if Dexcom should decide to 'retire' the G6 without making changes to the G7? I'm sure you've given this some thought and I would love to hear what your backup plan is.
Hello Dan. Well-written article. I don't remember how I discovered your substack but I sincerely appreciate your extensive research and ability to understandably present it to others with T1D. Your article on insulin pumps was fascinating, especially the benefits of pumps stratified by age groups. At 69 years of age, I am content with insulin pens for my diabetes management (last A1C was 5.7%) and that article confirmed that my approach was sufficient. But, I will still pay attention to diabetes technology and advances; perhaps I'll try a pump in the future. My best to you and I look forward to more of your articles.