


The Insulin Absorption Roller Coaster and What You Can Do
The T1D carnival’s scariest attraction is, weirdly, Insulin


Welcome to the T1D carnival's main attraction: the glycemic roller coaster! This thrilling ride of unpredictable highs and sudden, spiraling lows starts innocently enough. Just after dinner, your blood sugar rises slowly and surely, and when it gets to the top, it just hangs there. None of the insulin you’ve been taking seems to have any effect. And then, just as mysteriously, it all comes spiraling down at once. In minutes, you go from 350 mg/dL to 70, then 60, then 50, and now you’re stuffing your face with cotton candy, only to catch the next wave: The loop-d-loop! Your sugar’s up again! More insulin; you’re down again! Ice cream cones! You’re up again!
You’re nauseous.
Welcome to the weird world of T1D, the carnival of distortions, where fun-house mirrors, clowns and that wild glycemic roller coaster leave you feeling a bit woozy.
It’s easy to chalk up weird glucose excursions to all sorts of things: miscounted carbs, poor sleep, stress, and other legitimate factors. Yup, these things happen.
But there’s another explanation: insulin absorption variability. It’s the biggest secret hiding in plain sight, according to the literature review paper that analyzed hundreds of published papers dating back decades, Why 100-Years After the Discovery of Insulin and the Appearance of Insulin-Induced Lipodystrophy: Are We Still Struggling with this Nasty Complication?
The main point of the article is that lipodystrophy is the most consequential, yet rarely discussed aspect of T1D management.
I know what you’re thinking: “Lipo…What? Ok… what’s that?”
That’s what this article aims to cover, which may also help in avoiding the problem, which may earn you one small stuffed animal.
Insulin Absorption and Lipodystrophy
Let’s start at the beginning: When you’re new to T1D, your tissue is “naive” to insulin, in that it hasn’t been exposed to it for very long. The pristine tissue means that when you take insulin, you can pretty much expect it to take effect in a particular way. This is its absorption profile. Below is a common chart that shows long it takes for various insulin types to begin to act, how long till it peaks, and how long it can stay active in your system.
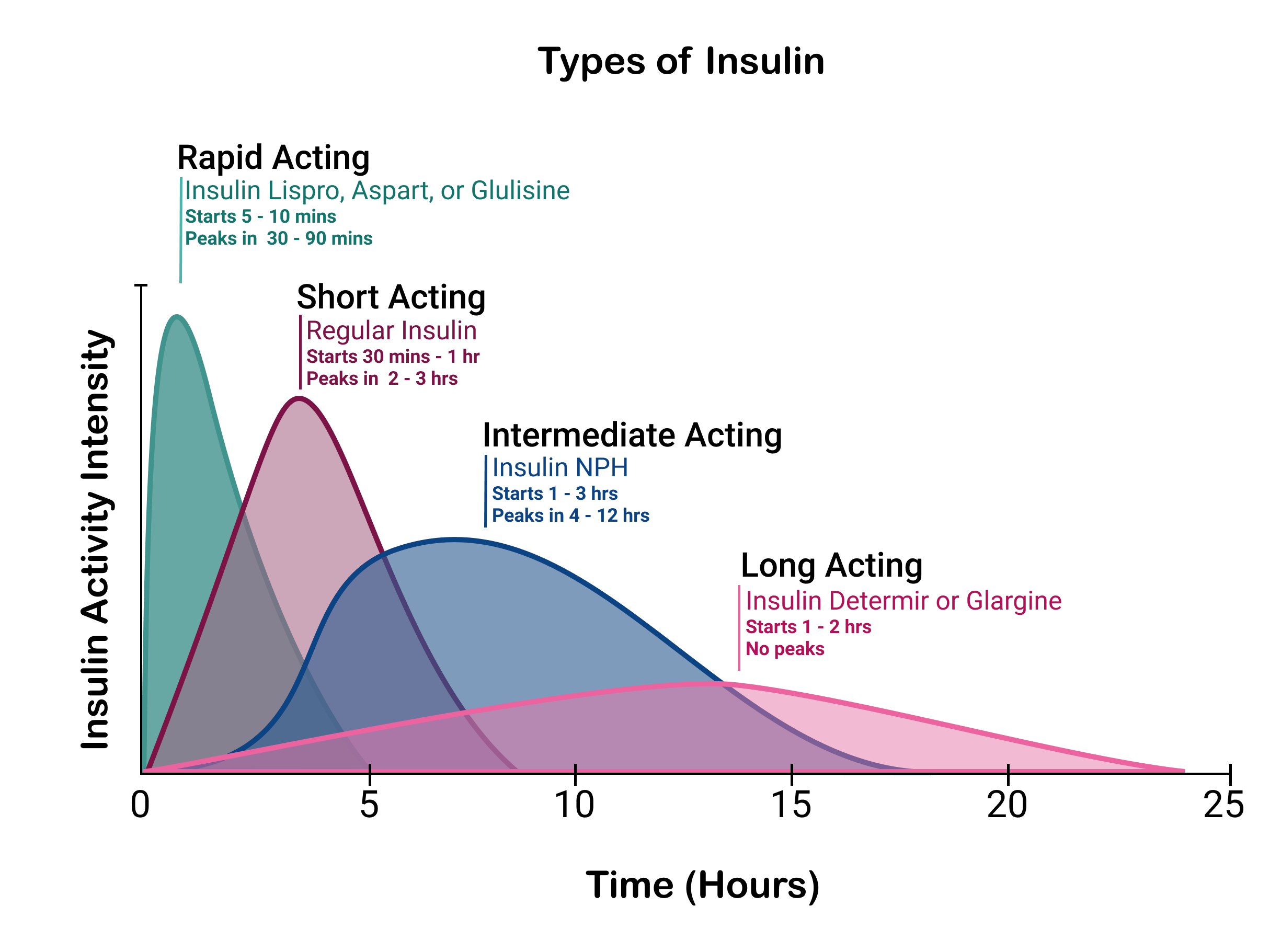
As this chart shows, different insulins have different profiles. These are published by companies that make insulin, and they drive everything you learn about T1D: Carb-to-insulin ratios, insulin dosing calculators, automated insulin pump algorithms, the “insulin-onboard” estimates you see in apps, and so on. Most everything people assume about T1D management is derived from these ideal conditions.
That is, these absorption profiles are established on (mostly) insulin-naive individuals in order to get good, clean data.
The problem is, the longer one has T1D, the tissue where insulin is administered generates an inflammatory response, affecting the way insulin is absorbed. That’s lipodystrophy, and it can manifest as either lipohypertrophy (thickening of fatty tissue) or lipoatrophy (thinning of tissue), both of which results in reduced blood flow to that location. That’s what changes the kinetics of absorption.
Over time, what used to be a rather smooth, predictable curve, insulin absorption becomes increasingly less predictable. And these curves don’t just shift to the right—absorption is not always “slower.” Rather, absorption profiles begin to “wobble”—fast, slow, stops-and-starts, herky-jerky. It’s the bumper cars at the carnival. Absorption starts falling into a more chaotic, randomized fashion. Insulin is still available and working, just not in the smooth, timely manner as it used to.
How long it takes or naive tissue to become damaged (and the degree of damage) depends on the quantity of insulin is delivered in any given location, the duration of administration, and the types of insulin used. You can change sites to newer, less used tissue to get a more regular, expected absorption response, but over time, you’ll eventually cover all the sites available on your body, and the erratic patterns never go away.
If that weren’t bad enough, it also occurs at the same time as another dysfunction has been slowly creeping up: Food absorption variability. Here, years of elevated glucose levels affect “gastric emptying”, the rate in which your stomach digests food. Here, your glucose levels won’t react to food as reliably as they used to either. For more on that, see my article on food absorption variability. (I’ll remind you again later.) This is the evil clown laughing at you inside the fun-house.
The worst scenario is when both insulin absorption and food absorption rates are both out of sync with one another. Virtually all unexpected highs, lows, confusion, rage boluses, panic eating, and other conditions that most T1Ds experience can be attributed to either or both of these conditions.
These dysfunctions happen to everyone over time—there’s no avoiding it. Nor can it be diagnostically measured. One day, you get one profile, another day yields different results. Again, this applies to both insulin and food absorption.
This also explains why automated insulin pumps can only achieve a particular level of performance: No matter how much an algorithm may try to analyze data and use historical context to predict insulin dosing, they cannot account for the in-the-moment variability in food and insulin absorption. Those factors are too stochastic (random) to reliably factor into equations.
This is why those who perform the best with automation are children and recently diagnosed—they haven’t yet developed enough of these physiological dysfunctions to cause lipodystrophy or food absorption problems. Accordingly, most studies you see that show the benefits of insulin pumps are always using idealized candidates: People who have not developed food or insulin variability (children up to young adults), OR people who are either unable or unwilling to self-manage themselves (not a small group of people).
For everyone else, the performance of automation is a mixed bag, depending on an array of factors. A complete analysis can be found in my article, Benefits and Risks of Insulin Pumps and Closed-Loop Delivery Systems, and be prepared to see some real-world studies that weren’t funded by pump companies.
By no means am I suggesting that insulin pumps or automated systems are “bad.” Look, T1D is a tough disease, and sometimes, it’s a choice between a lot of bad options. These systems make things easy, and for some, “easy is better than good.” But one should also not be under the illusion that automation is better than what you can do on your own, provided you learn important habits. (You can read about them here.)
The variability of insulin and food absorption also affects other tools that T1Ds use, such as insulin dosing calculators. The FDA had always been highly resistant to approving them at all for these reasons. But a single key argument won out: Newly diagnosed T1Ds are so bewildered about how to dose insulin, that something was better than nothing, especially since their food and insulin variability had not yet set in. “Bolus calculators”, as they are also called, have since been endorsed, and are incorporated into various automated systems, with many forgetting that such formulas’ efficacy wanes as food and absorption variability set in.
The same can be said of “insulin on board” and “carbs on board” indicators in some T1D apps.
For those who’ve had T1D longer than 5-10 years or so, they can be dangerously untrustworthy. They will be wrong far more often than right. But the young and newly diagnosed, they’re useful tools.
So, what can you do about lipodystrophy? Is T1D so random that we should just give up?
Obviously not. But it requires a tiny serving of education (I’ll make it easy), and a shift in T1D behaviors. (Also not hard, but requires willingness.)
By understanding how insulin gets absorbed in the first place, we set the stage for how to modify behaviors to improve glycemic control.
Injection Method: Subcutaneous (SC)
This is the part most people focus on: how insulin moves from the site of administration into the bloodstream. From the time of their initial diagnosis, T1Ds are taught to inject insulin into subcutaneous (SC) tissue, specifically, the abdomen, because there’s better blood flow in that area. This is the case, whether they start with pumps or insulin pens or syringes (“Multiple Daily Injections”, or MDI).
In both cases, they are also told to “rotate injection sites”, which means avoiding taking insulin in or near the same spot very often. This is to avoid lipodystrophy.
For those on MDI, it’s easier to rotate sites because each injection is done independently. You can take a morning dose in the abdomen, lunch in the arm, and dinner in the leg. This wider distribution of insulin into tissue limits the amount of insulin at one location, while also providing considerable time to heal till the next time that site is used.
Unfortunately, those using pumps don’t have this flexibility. Because an infusion set remains in a single location for days at a time, the amount of insulin affecting that tissue is orders of magnitude more than that of a single injection using MDI. And because of the volume disparity between a pump and MDI, the amount of time needed for a pump user to develop lipohypertrophy is much shorter.
This was explored by researchers in a paper that specifically looked at children, The Impact of Insulin-Induced Lipodystrophy on Glycemic Variability in Pediatric Patients with Type 1 Diabetes. Here, researchers compared the rates of lipodystrophy based on method of insulin administration (pump vs. MDI), and other factors (age, years of T1D, gender, etc.). Children who start on pumps at very early ages can experience tissue damage within months, compared to MDI users where damage can take between 5-10 years to set in. Unfortunately, some pump manufacturers are looking to expand the life of an infusion set from three to seven days, so the problem is likely to get worse for pump users.
It’s not just lipodystrophy—it’s level of engagement with their self-management. In a study titled, Impact of Insulin Injection and Infusion Routines on Lipohypertrophy and Glycemic Control in Children and Adults with Diabetes, the study subjects (both MDI and pump users) were observed and instructed to engage in site rotation, and found that MDI site rotation resulted in better glycemic control and lower incidence of lipodystrophy, largely because they were more attentive to their dosing.
Another problem for pumps is that when the tissue is damaged, the less accurately the pump itself can push the intended amount of insulin. This phenomenon is detailed in the 2022 peer-reviewed paper, Insulin induces a progressive increase in the resistance of subcutaneous tissue to fluid flow: Implications for insulin pump therapy. Here, the authors set up a study consisting of thirty T1Ds wearing two Accu‐Chek Spirit Combo insulin pumps. One pump used actual insulin, while the other used an insulin diluting medium. The pressure in all the pumps was measured as the days progressed, and the authors found that the pressure associated with pumps using insulin had dropped significantly, versus pumps using the diluting medium, which remained constant. (For a more detailed discussion on this, see my article, Conditions Where Insulin Pumps May Not Deliver Intended Doses.)
If all of this sounds like pumps are bad or ill-advised, it’s not. All of these problems can be mitigated with other techniques and behaviors discussed later.
Injection Method: Intramuscular (IM)
While lipodystrophy can be mitigated by rotating sites in SC tissue, there’s another method of injection that is far less susceptible to lipodystrophy, and can also vastly increase the absorption rate: injecting directly into muscle tissue. This method is not widely used (largely because people are unfamiliar with it), and docs are apprehensive to recommend it for reasons you’ll quickly understand. (It also cannot be done with insulin pumps—only syringes or pens.)
Intramuscular (IM) injection has a very rapid absorption profile because the target tissue is highly vascularized, allowing insulin to be absorbed directly into the bloodstream much more quickly than SC. Decades of studies show that IM injections are found to reach peak concentration up to 50% faster than SC injections and have a shorter time to onset by nearly 30 minutes.
One study is profiled in the article, Intramuscular injection of insulin lispro or soluble human insulin: pharmacokinetics and glucodynamics in Type 2 diabetes, which showed that IM injection of insulin lispro (Humalog) yields a stronger metabolic effect in the first two hours, compared with SC injection. I chose to highlight this study over others because T2Ds exhibit a more similar insulin-resistant profile to the conditions we’re concerned about: Variability of insulin absorption.
So, what’s the problem with IM injections?
For one, IM injections rely on actually using the muscle you inject into. If you don’t move the muscle, absorption rates can be slower. But now that you know, it’s not a big ask to “move the muscle.” This isn’t exercise, per se. It’s just movement. Thigh muscles are best because they’re larger and more vascularized; upper arms are also good. Simply put, inject and move around.
Also remember, muscle movement also takes up glucose, independently of insulin. So, if you inject into a thigh muscle and then walk (or peddle on a stationary bike, e.g.), both the muscle movement and the more rapid absorption of insulin not only reduces glucose levels faster, but less insulin is required to do that same job, compared to SC injections. So, you would need to dose accordingly. Usually, less, but your particular profile can only be determined by trial and error. (Learning how to manage insulin and exercise is itself a whole nother topic, which I cover in my article, The Paradox of Low-Carb Diets: A1c vs. Metabolic Health.)
Another concern is that it’s not always easy to hit a muscle for some people. Given that most insulin needles are 5mm to 8mm, many may find it hard to penetrate deep enough through the outer layer of adipose fat tissue.
Lastly, it’s not necessarily the case that muscle tissue doesn’t get lipodystrophy or other kinds of damage. It’s just that it’s more resilient than SC tissue and the damage can recover faster.
Again, all these caveats aren’t “bad” per se. It’s just complicated. You can see why docs would be apprehensive to discuss this during a 15 minute appointment. But it might be a very useful technique for pump users who want to address that stubbornly high glucose right after dinner.
Insulin Types
The type of insulin used also affects lipodystrophy. Human Insulins (Regular and NPH) accelerate lipodystrophy much faster and worse, whereas rapid-acting insulin analogs (e.g., Lispro, Aspart, Glulisine) are marginally better.
The design improvements for these “faster” insulins, which include Fiasp, etc., are to formulate them in a way that the insulin molecule itself is more isolated from others: E.g., dimers (two molecules) instead of hexamers (five molecules). Insulin cannot work until it’s a single molecule, so the “dimer” can separate more quickly than the hexamer—hence, it enters the bloodstream sooner.
While these insulins take effect a tad faster, they are no better or worse insofar as lipodystrophy. In fact, once someone’s lipodystrophy advances, the faster profile is less pronounced. T1Ds with more lipodystrophy might not see much difference at all between faster and more traditional insulins, whereas those with less lipodystrophy will see those differences.
That said, injecting into muscle tissue yields a much faster effect profile because there’s less chance of lipodystrophy in these regions.
Long-Acting Insulin Analogs (e.g., Glargine, Detemir, Degludec) are formulated in ways that slow absorption rates in order to provide a steady “basal rate” of insulin delivery. These insulins definitely go slower, but their formulation increases inflammation and lipodystrophy, making that slow release increasingly volatile. Case studies show that people who get off of Lantus (glargine) can experience residual insulin effects for days after termination.
NOTE: The variability of long-acting insulins, combined with the variability of boluses you take for meals, combined with food absorption variability makes for a very challenging glycemic control situation, setting the stage for a potentially faster and scarier roller coaster ride.
“Smart insulins”
New efforts are being investigated for “glucose-responsive” insulin, or GRI (also called “smart insulin”). These are designed to act dynamically, sensing glucose levels and releasing insulin accordingly. The technique involves attaching glucose-sensitive chemical groups to the insulin molecules. When glucose levels rise, glucose molecules bind to the glucose-sensitive chemical groups, releasing insulin. As glucose levels normalize, glucose molecules dissociate, slowing or stopping further insulin release. Hypothetically, you only get the insulin you need proportional to your glucose levels.
There are numerous difficulties with this approach, but the biggest practical roadblock is the physiological reality of muscle glucose uptake. As noted earlier, muscle uptake of glucose without insulin mediation means that your systemic glucose levels will never be high enough to do any exercise. A GRI would keep insulin levels too low to properly engage in a healthy exercise regimen.
Inhaled Insulin (Afrezza)
One way to get around the whole bottleneck of tissue absorption problems is to just go directly into the bloodstream, and one product that does this is Afrezza—inhaled insulin—which goes into blood through the lungs. The absorption profile for Afrezza is, not surprisingly, similar to IM injections.
Just as IM has caveats, so does Afrezza:
Afrezza dosing increments are large and lack fine granularity.
It may not last long enough to cover meals with extended absorption (think high-fat, high-protein meals), which may take multiple doses to get precision.
Long-term pulmonary safety data is still limited.
Risk of hypoglycemia is on par with IM injections, especially for those who are on (unnecessarily high) basal rates. (Another reason to reduce basal dosing.)
As for efficacy, the INHALE-3 study showed that those who used Afrezza over the course of 30 weeks had neutral results: 26% the group’s A1c improved by .5%, while the same number worsened by .5%. The remainder didn’t find any change. Perhaps the most concerning aspect from this study is that the study group’s total daily insulin increased from 36u at 4 days to 48u at 17 weeks and 52u at 30 weeks. This is a rather large increase in total insulin, especially given that the change in A1c levels was largely negligible.
Afrezza has its fanbase, and can be a very useful tool for those excruciating highs where you can’t exercise at all (like a long drive, sitting in meetings, a flight, or before bed). But IM might be easier and allows more precise dosing.
Other factors affecting insulin absorption
Besides the type of insulin and the nature in which its delivered, other factors can affect absorption variability.
Large doses of insulin absorb more slowly than smaller doses. The kinetics of how insulin diffuses in order to enter the bloodstream is such that the smaller the dose, the quicker the absorption. For MDI users, taking smaller boluses is best. Many use a rule-of-thumb to never inject more than 5u in one injection. If you need more, break it up into several injections and use a different site for each one.
It would seem that pump users win out here, because the steady “drip” (basal rate) involves sub-unit doses. The problem is, it’s all still going into the same spot, so the tissue itself can have insulin “pools”. This isn’t entirely noticeable—and again, it’s stochastic. If the rate of entry is roughly the same as the rate of exit, the disparities smooth out…until they don’t. The moment something happens that jiggers that pool, a sudden release can quickly move glucose levels down, and, well, get ready for the next roller coaster. You’re first in line to board.
One such trigger is heat. Warmer tissue means more and faster blood flow, and faster insulin absorption. Cold? Expect delays. If there’s pooled up insulin—or worse, basal insulin (like Lantus)—this quick release can put you in the front car of the glycemic roller coaster. Not fun.
For smaller boluses, one way to increase absorption is to apply a warm compress to the injection area for a few minutes before or after injecting (MDI only). Also, take advantage of post-shower warmth—just don’t overheat the insulin itself.
Remember, insulin starts degrading rapidly above 86°F (30°C). Warm the site, not the insulin.
Note that insulin does not have to be refrigerated all the time (studies show that it can survive in “room temperature” for up to 60 days), but insulin degrades rapidly above 86°F, so be careful exposing insulin for extended periods of time when outside on hot days.
Heat exposure is particularly concerning for pump users who spend a lot of time outside during summer months because the reservoir is exposed to ambient air. The paper, Characterizing normal-use temperature conditions of pumped insulin, cites studies that show that insulin pump reservoirs can experience temperatures ranging from 25°C to 37°C (77°F to 98.6°F) during normal use, regardless of the season. Heat-exposed insulin in pumps can lead to the onset of DKA, which case studies show happens far more frequently in the summer months. This is yet another reason to change infusion sets frequently.
MDI users should keep insulin cool when outside on hot days by using cooling pouches or cases. (I personally carry my insulin pen in my fanny pack with a cold drink inside when hiking in hot weather.)
Some final words…
There may be those who feel they’re doing just fine and they’ve had T1D for 25+ years. Indeed: As I mentioned before, behaviors have a greater effect on outcomes than the absorption variability discussed here. Exercise, for example, can do wonders. Even a 10 minute walk after a meal can dramatically reduce the amount of insulin needed for for that food. Exercise has been shown to reduce inflammation, improve blood circulation, reduce insulin resistance, increase insulin sensitivity, and improve metabolic health, all of which contribute to more efficient insulin absorption, even in the presence of lipodystrophy.
There are other “habits” that also contribute to healthy glycemic control that can override or mitigate absorption variability. In my article, The Four Habits of Healthy T1Ds, those who engage with their diabetes employ these habits to good effect.
Habit #1 is: Pay attention to your CGM. The earlier you can catch unexpected movements, the better able you are to respond proactively. A meal bolus may possibly be best handled by several, smaller, incremental doses 30 minutes apart from one another. If you do this using an insulin pen and inject into the muscle, you’ll get far more reliable and predictable absorption rates, while also being highly aware of those anomalous situations. Sure, things go wrong from time to time, but when you pay attention, they are far less severe, and more easily remedied.
Lastly, as promised, here’s a reminder to read my article on food absorption variability, and how to avoid it. It also covers the best way to treat hypoglycemia.
The roller coaster has now stopped. Gather your belongings and exit the ramp. Enjoy your time at the carnival.
Awesome article that I feel I've been waiting YEARS to read. Every day is a roller coaster after almost sixty years of type one. It is a combination of watching my cgm like a hawkn despite its occasional irregularities and inaccurate readings, and using affreza, when things really go insane (not quite daily). My control is excellent but that is really only because I regard control as a full time job, in addition to my regular full time job. (-: Thanks so much for all you do for this community.
Very interesting article. I move from MDI to a tandem pump during the year. Was on MDI for about three years. Just went back on pump for travel. Easier for me. When on pump I change infusion site every two days and use steel cannulas. When on MDI I will use IM injection to bring down BS faster. Didn’t occur to me to use muscle all the time. May have to try when I switch. Thanks for all of your information. Just had too much desert at a party. Went for a two mile walk and all back to normal. Oh and I don’t use the tandem controlIQ. So not at the mercy of an algorithm