
Why Controlling Glucose is so Tricky
Hint: Even the natural human body struggles with it in strange and unexpected ways.


Key Points:
Insulin is the primary mediator for disposing glucose from the bloodstream into cells that need energy, but it’s only one of 15 mechanisms that do this.
What’s more, the rate and frequency of those other hormones are inconsistent, amplifying the variability of glucose levels, making it even hard to predict how much insulin may be actually needed at any given time.
Muscles are the primary consumer of glucose, and they can uptake glucose both with and without insulin mediation. And that variability is also, well, variable.
With all this variability beyond insulin in lowering glucose levels, knowing how much you should dose at any given time is like trying to use a bow and arrow to hit a target 5 meters away during a windy and rainy day. Gaining a sense of that wind is more of an art than a science, and that’s where T1D management goes from “ok” to “good,” or even “great.”
This challenge is not limited to T1Ds—these physiological features are part of how the human body works, and given the rise in type 2 diabetes, it’s evident that the body has its own limits on how well it can manage glucose levels.
The best solution for everyone—T1Ds and others—is to engage in healthy activities that optimize the efficacy and efficiency of glucose metabolization, thereby making the dosing of insulin more precise and effective.
Most people seem to think that someone without diabetes has perfect glucose control, so it’s just a matter of simulating ideal insulin delivery based on glucose levels.
It’s not that simple.
Glucose in the bloodstream is not merely a byproduct of having eaten food—your body makes it too. And insulin isn’t the only hormone that draws glucose out of the bloodstream—there are 14 other hormones that do that same job, and those function just fine in T1Ds as well.
The challenge for T1Ds managing blood sugar is not as simple as dosing insulin for specific glucose levels, because those other mechanisms are also at work. So, when dosing for insulin, it’s useful to know more than just what your glucose levels are—it also helps to know the conditions of the moment.
Needless to say, this is not easy. As we’ll discover, even the natural human body has a very hard time maintaining glucose levels. That said, the goal isn’t to be perfect; it’s to be “good enough.”
We begin with the basic question: Just how much glucose is there inside us?
How much glucose is in your bloodstream?
Let’s start with a perspective that may be shockingly simple: The average person has between four and five liters of blood, so a “normal” blood glucose level of 100 mg/dL means that a typical person has about one teaspoon of sugar throughout their entire bloodstream. That’s a whopping 4.2g of glucose. Here’s a visual representation, brought to you by AI.
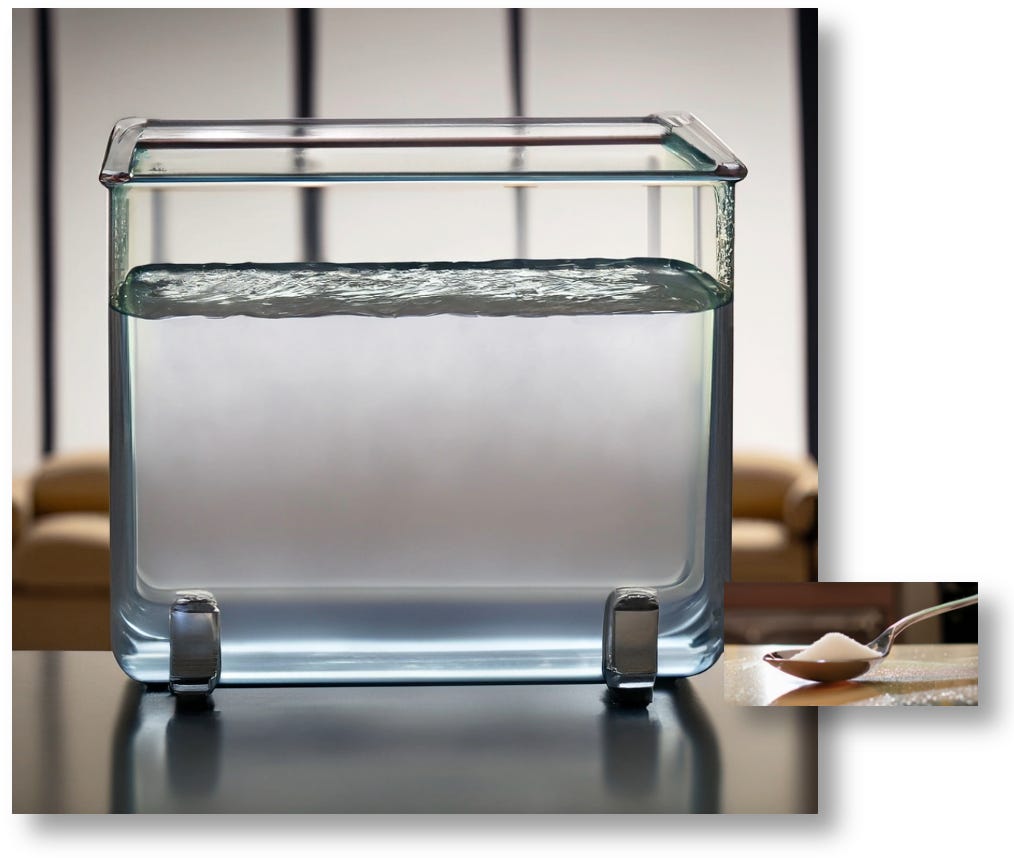
As you can see, 4.2g of glucose is proportionally tiny to the total volume of fluid. If you were to add 2.1g of glucose—a half a teaspoon of sugar—the total glucose content of this beaker would grow to 140 mg/dL.
But as any diabetic can affirm, eating a half teaspoon of sugar isn’t going to raise glucose levels to 140. So, where is all that glucose going?
As we’ll see in this article, the body shuttles glucose around to different organs, often without the aid of insulin. What’s more, we also have hormones that cause the body to create glucose and deposit into our bloodstream (often, even if we don’t technically “need” it). This is an ongoing process, and incalculably complex.
This is why keeping glucose levels stable is incredibly difficult, even for perfectly healthy individuals. In fact, when we examine how non-diabetics metabolize glucose, we often see the same variability as we T1Ds see in our own glucose levels. We’ll look at those graphs soon enough.
Why do glucose levels vary so much, and so rapidly?
Research shows that our 3-5 pounds of brain matter holds 20% of the body’s total glucose volume at any given time, and it burns ~78.4 mg of glucose per minute. That’s about 1g of glucose every 12 minutes. And yet, insulin is not involved in the brain’s metabolization of glucose. Think about that for a minute. (Whoops, you just consumed another chunk of glucose!)
In fact, many organs get glucose from the bloodstream without insulin mediation. Interestingly, the kidneys filter and dispose of glucose too, although the rate varies considerably by individual, time of day, metabolic conditions, and so on. This is an unpredictable process.
One of the biggest consumers of glucose are our muscles, but here’s where insulin’s role also has variability. Depending on the level of exertion and the “fitness” of the muscle fibers, glucose can be drawn directly from the bloodstream with and without insulin mediation—that is, a combination of both. Suffice to say, if you don’t exercise very much, muscles depend almost entirely on insulin to get their glucose.
And this consequently makes for a very sad and unfortunate reality: The less you exercise, the easier it is to control glucose levels if you take insulin. But the paradox is that exercise is so healthy for you, that by not exercising, you’re doing more harm to yourself than the small amount of benefit you may get from the “easier” management of glucose levels.
For more on that, see my articles “T1D and Health: How Long Will You Live?”, and “The Paradox of Low-Carb Diets: A1c vs. Metabolic Health.”
Managing glucose with exercise is only more difficult because it’s not explained or taught by a typical medical practice. But, the technicality is not really that hard, and once you know how glucose is actually metabolized, insulin management becomes easier. That’s covered a bit in those two articles, but I’ll write more about it in the future.
After all those things we just covered, whatever glucose is still leftover in the bloodstream is converted into fat as “storage,” and that process can only be done by insulin.
The goal here is not to detail all those processes precisely, only to expose you to the vast complexity of the human body.
Next is understanding how glucose is moved around, as that will help move this along.
Glucose Transporters
The means by which glucose moves from the bloodstream into cells is through little portals that are activated by “glucose transporters.” Among the many glucose transporters in our bodies, insulin activates glucose transporter #4, also called GLUT4. When the insulin molecule lands on a given cell, the GLUT4 transporter rises to the surface of the cell, opening a portal that allows glucose to passively enter from the bloodstream.
Insulin only activates the GLUT4 transporter, but there are many such transporters, all of which can siphon glucose out of the bloodstream as well. And again, insulin isn’t involved in those processes. The full list of glucose transporters can be found in this paper published in BioPhysical Reviews called, “Glucose transporters: physiological and pathological roles.”
Here's a summary of some of the most well-known ones:
GLUT1: This is a widely expressed glucose transporter found in most tissues, including red blood cells, the brain, and the placenta. It's responsible for basal glucose uptake, meaning it provides a constant supply of glucose to cells for basic metabolic needs.
GLUT2: This transporter is primarily found in the liver, pancreas, and small intestine. In the pancreas, it plays a key role in glucose sensing by beta cells, which are responsible for insulin secretion. In the liver and small intestine, it's involved in glucose transport. (In T1Ds who have very few working beta cells, the GLUT2 transporter is still functioning; it’s just that there may not be enough beta cells to respond.)
GLUT3: This is the main glucose transporter in neurons. It has a high affinity for glucose, ensuring that neurons have a constant supply of energy even when glucose levels are low.
GLUT5: This transporter is different from the others because it primarily transports fructose, not glucose. It's found in the small intestine and plays a role in fructose absorption.
In addition to these, there are other GLUT transporters with more specialized roles:
GLUT6: Found in the brain, spleen, and leukocytes (white blood cells).
GLUT7: Found in the small and large intestine, transporting glucose out of the endoplasmic reticulum.
GLUT8: Found in various tissues, including the testis, brain, and liver.
GLUT9: Found in the kidney, liver, and other tissues; also involved in uric acid transport.
GLUT10: Found in the liver, pancreas, and other tissues.
GLUT11: Found in the heart and skeletal muscle.
GLUT12: Found in muscle and other tissues.
GLUT13 (HMIT): Primarily expressed in the brain and transports myo-inositol.
GLUT14: Found in the testis.
See how complicated this is getting? Regulating glucose involves a lot of things going on at once, and each one of them is volatile and inconsistent. So, what happens if we don’t have enough—or too much—glucose in our bloodstream?
Counter-regulatory responses
Given all the mechanisms that uptake glucose from the bloodstream, it’s pretty evident that any disruption to that process can be devastating, as each of our organs need glucose to function. Once glucose levels get out of balance, higher or lower, the body produces a cascade of other hormones in its attempt to restabilize glucose levels. And that chain reaction is highly unpredictable and volatile too, even for the natural human body.
In the article, “The Six Dysfunctional Hormones of Type 1 Diabetes,” the author reminds us of other essential cells that produce hormones that that keep glucose levels in check. Remember, beta cells reside within islets alongside several other cells that all work together to release hormones that regulate glucose levels. T1D is caused by beta cells having been destroyed by the immune system, but the other cells that reside within the same islets are still intact and functioning, although their efficacy is impacted by the beta cells’ inability to produce insulin and amylin, which are signaling hormones for other biological functions. More on that in a sec, but first, the other cells are:
Alpha cells, which produce glucagon, signal the liver to produce glucose (gluconeogenesis) to help avert hypoglycemia, among other things.
Beta cells also produce amylin, which works with both insulin and glucagon in cell receptors to aid in glucose stabilization. Amylin slows gastric emptying (the rate at which food empties from the stomach into the small intestine), which helps to prevent rapid spikes in blood sugar after meals. T1Ds won’t get this benefit, so gastric emptying is not slowed, resulting in a faster rate in blood glucose levels. Moreover, amylin suppresses the function of Alpha cells’ secretion of glucagon, which helps non-diabetics keep glucose levels stable (but so do delta cells). Lastly, amylin promotes feelings of fullness, which can help to regulate food intake.
Delta cells produce somatostatin, which inhibits the secretion of both glucagon and insulin to maintain glucose homeostasis. For T1Ds, delta cells can assume some control over the suppression of glucagon that amylin is not able to do.
Gamma cells produce pancreatic polypeptide, an important regulator of glycogen storage in the liver, also enhances insulin sensitivity.
Epsilon cells produce Ghrelin, which stimulates appetite and growth hormone release from the pituitary gland.
Each of these cells are integral to the larger constellation of signaling hormones that are essential to glucose regulation. One can’t just expect to regulate glucose by dosing insulin in response to blood glucose levels the way we expect a future automated insulin pump to work.
And those are just the hormones inside the pancreas. Once you get into other areas of the body, the entire system gets even more complex.
This diaTribe article enumerates 22 factors that affect glucose levels that can affect even more hormone imbalances. Examples include things like medication, sickness, infections, poor sleep, or even the simple task of being a kid. (If you have a teenager, or have seen one on TV, you may have observed what happens when hormone activity goes awry. Now imagine their glucose levels.)
Why is it necessary to keep glucose levels low and stable?
This is a question too few people ask because it seems obvious, but the answer isn’t just “interesting,” it also raises a perplexing paradox: Excess glucose can be toxic, but too much insulin can be just as bad.
Let’s begin with what happens when glucose levels increase to 140-160 mg/dL (A1c of 6.5% and higher). This is the tipping point where glucose causes proteins to get sticky (glycosylation), and begin obscuring the narrowest part of the vascular system, beginning with the tiniest capillaries. Sticky proteins make it hard to deliver oxygen to tissues, leading to things like retinopathy (which leads to blindness), nerve damage, and other problems. This is why infections take a long time to heal.
As time passes, increased glucose levels affect progressively larger organs, such as the liver, kidneys, heart and vascular system.
Glucose is also very abrasive. When too much glucose is in the bloodstream for extended periods of time, it affects the lining of veins, rapidly increasing the risk of atherosclerotic cardiovascular disease (ASCVD), which happens to be the leading cause of death in America. Highly elevated glucose levels just accelerates the process, which is exactly why T1D life expectancy is 10-15 years sooner than non-diabetics. You can read more about it in this 2016 article in the journal, Circulation, “The Prediction of Atherosclerotic Cardiovascular Disease in Type 1 Diabetes Mellitus.”
The toxic effects from glucose on the body explain why diabetes is defined as having a 90-day average glucose level at or above 140 mg/dL, because that’s when damage begins.
By the way, when you think of the “normal” glucose range is 70-180 mg/dL, that’s because these are the levels found among the general population of non-diabetic individuals. Now that you know that 140 is where things go awry, why would a non-diabetic regulatory system allow levels to get to 180? And why is that “normal?”
The short answer is, it doesn’t want to! And normal is certainly not healthy. Keep that in mind!
The metabolic system tries very hard to keep glucose levels lower, but again, our lifestyle choices overwhelm the body’s regulatory limits.
Glucose levels under 140 is necessary to experience fewer complications and live longer lives, but people’s lifestyles are such that they exceed those levels, and the natural human body can’t compensate. The only way to achieve those levels is to work at it by eating less and exercising more. (More on that later.)
With this context, let’s look at CGM patterns for non-diabetic adults, and get a closer look at what the body is trying to do to keep glucose levels stable.
Non-diabetic glucose patterns are problematic
One of the benefits of CGMs is the ability for researchers to get an accurate picture of the glucose patterns in otherwise healthy, non-diabetic individuals under various controlled and real-world conditions. Here’s a hint: It ain’t pretty.
This 2015 study from Stanford University involved healthy, non-diabetic subjects being given exactly the same food and activities at the same time each day for two weeks. And yet, researchers found large variations in blood sugar levels, as shown by the following chart of three individuals involved in the study.

The study has been replicated over the years since, involving thousands of similarly healthy individuals, all with similar outcomes. The lesson we learn is that, even when under the most restricted control, glucose levels swing in volatile and unexpected ways among otherwise healthy non-diabetic individuals.
Naturally, one would expect that diet can adjust for such volatility, but, once again, it’s not that simple. It’s not just about glucose control or carbohydrate intake, but the availability of sufficient balance of carbohydrates, protein and vitamins. Each of these also has an effect on glycemic control, not just one. For example, consider this 4-day glucose patterns of a healthy non-diabetic on a ketogenic diet.

Glucose variability (GV) is a direct byproduct of the metabolic system attempting to keep glucose stable against the turmoil of counter-regulatory hormones triggered by changes in diet, the environment, pathogens, and even just emotions. That very turmoil is itself unhealthy. In the study titled, “Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients,” the authors write, “… oscillating glucose can have more deleterious effects than constant high glucose on endothelial function and oxidative stress, two key players in favoring cardiovascular complications in diabetes.”
Since that study showed effects on non-diabetic subjects as well, all the more reason why T1Ds should be even more conscientious about their glucose variability.
Believe it or not, this is a good thing, because it also illustrates the metabolic system’s adaptability. As food types and sources change, the metabolic system adjusts itself to react accordingly. If it didn’t, we wouldn’t survive periods of famine, extreme heat or cold, running after (or away from) wild animals, or even the process of procreating. (Keep those hormones in check, dear reader.) But the whole thing is also a double-edged sword, too, and insulin is the culprit.
Why too much insulin is bad
Since we’re talking about insulin, let’s talk about why too much of it can also be bad, even for non-diabetics. While it’s essential for clearing glucose from the bloodstream, insulin is also the primary shuttle for excess glucose to be stored as fat. Yes, that ugly stuff.
There are many different types of fat, but the one we’re concerned about is visceral fat. This is not what you see around your torso or under the skin, nor is it in the foods you eat. It’s the type that surrounds internal organs, including the stomach, liver, kidneys, heart, muscles and intestines, and it’s made entirely because of insulin’s interaction with the GLUT4 transporter. As insulin clears out excess glucose from the bloodstream, it progressively builds more and more visceral fat, which leads to inflammation, and ultimately, a degradation of performance of all these organs.
In the body’s attempt to keep the amount of visceral fat from accumulating, the fat becomes a primary source of insulin resistance, which again, is another wonder of the metabolic system’s adaptability, but also presents a flaw. The resistance keeps more fat from being made, but it also keeps that glucose in the bloodstream, which is also bad. It’s a no-win situation.
Ideally, the person would reduce caloric intake, but many people find that difficult, so as more carbs enter the bloodstream, the body makes more insulin (or the T1D injects it) which makes more fat, increasing insulin resistance, which then requires even more insulin to keep blood glucose levels down. As the feedback loop accelerates, we get to obesity.
This might make it abundantly clear now: If the natural body were so good at managing glucose levels, there wouldn’t be 40 million type 2 diabetics in America, with another 98 million undiagnosed. Insofar as T2D is concerned, this feedback loop happens without any symptoms at all, because while that fat accumulates, blood glucose levels remain low and stable. Of course. A non-diabetic body makes its own insulin, and so long as it can, fat just accumulates by removing excess glucose. One doesn’t know they’re becoming a T2D until the beta cells finally fatigue to the point where they can no longer produce enough insulin to overcome the resistance. When that happens, A1c levels finally start to rise, and the diagnosis is made. But by then, the disease had already been present—usually, over the course of years—so treating it becomes its own set of challenges.
The sad part is, T1Ds are following exactly this pattern: As I’ve written before, T1Ds’ singular aim of lowering their A1c levels has resulted in their taking too much insulin, raising the rate of obesity and along with it, many of the same metabolic disorders as T2Ds—a term now called “double diabetes.”
It’s easier to see insulin resistance in T1Ds because we can measure the rate of increase of insulin intake over time (and weight gain along with it). Any T1D who’s overweight must have some degree of insulin resistance.
To foreshadow one of the main drawbacks of automated insulin pumps is that the algorithms cannot assess—or make a judgment about—insulin resistance. They can only look at blood glucose levels (via a CGM), and will do as told: Keep those levels lower by administering insulin, even if it generates more fat.
And since pumps cannot detect any of the other hormonal activity going on, it’s going to err on the side of giving more insulin than less. Of course, the user can override that and keep target glucose levels higher, but then you’re going to have the problem with excess glucose: toxicity.
This is, once again, why the user must be engaged in their personal health. The best way to clear glucose from the bloodstream is physical exercise. It not only activates GLUT4 transporters on its own (with increased exertion), thereby reducing insulin requirements, but exercise also assists in converting visceral fat back into glucose so it can be used for energy. Exercise also builds new muscle fibers and mitochondria, which improves the volume and efficiency of glucose clearance from the bloodstream. Exercise can also reduce appetite (depending on aerobic fitness), making it easier to eat less, further reducing glucose, while improving cardiac performance, relieving stress on the liver and kidneys, improving sleep, emotions, and sexual health. (We’re adults here, right?)
Of course, we know that exercise isn’t that easy for anyone, much less T1Ds. Hypoglycemia (and the fear of it) keeps many from even starting exercise. It’s a complicated process, because insulin reduction rates vary, so one has to go about it intelligently. And automated pumps perform particularly badly with exercise, because they are not “adaptable” the way your body is; your past glucose patterns will definitely not apply to future outcomes. It just has to be done manually.
The best way to get started is remarkably simple: walk for 15+ minutes after meals. A tiny effort goes a long way. Most people who do this find their insulin requirements drop steadily. If they ramp up to faster walking or even light jogging, weight is reduced and glucose volatility drops too. From there, you might find that managing T1D isn’t actually “hard" (as it pertains to tasks). It’s just a matter of bothering to do it. You can read more about my journey in my article, “Why I Haven’t Died Yet: My Fifty Years with Diabetes.”
I haven't found the distinction you make, Dan, between the Tandem Tslim with Control IQ - a rules-based automated insulin pump - and using a manual pump. I wouldn't go back to any non-automated pump for anything, because it takes away a lot - but by no means all - of the many decisions we need to make each day, even each hour about insulin, carbs, exercise, ... Often from careful observation of what happens in recurring situations, I can do a small boost of insulin or suspend way before the pump does. The automated pump has improved my control but decreased the mental load a lot, so this has improved my mental health a lot. And no more ambulances in the middle of the night from the unexpected low from which I cannot be aroused without drastic intervention. And Control IQ is way better than Basal IQ or manual at dealing with overnight. Mostly I'm between 4 and 6 all night and sleeping all the time.
Wow....great article and here I am, with my new 780 pump being shipped, as of this morning!! I am so interested in the human input for a Type 1 in terms of managing. I have had diabetes for 73 years but have been on insulin pumps since 2000 and CGMs since around 2015. I've had my A1cs in the low 5's for most of my pump years. I use very small amounts of TDD insulin (11-13 units). I am horrified with the idea of "because you are an older person your blood sugars should run higher." As if I'm too old for something like a complication to finally appear...LOL. YES, I am very healthy. So I'm being pushed into using the Medtronic sensor system. Can it really manage ME better than I have been doing? I am keeping your article handy!!!