


Four Essential Diabetes Facts You Never Knew
Politics and Diabetes have a lot in common, but only one is easy to fix


The CDC has declared November as Diabetes Awareness Month, whose mission is “to bring attention to diabetes [and] taking action to prevent diabetes health problems.” And it’s the perfect time of year, too, since Thanksgiving is when I remind my dinner guests that we, as a country, can set aside our divisions and come together to peacefully and rationally talk about ways we can take better care of our diabetes.
You see, unlike politics, diabetes can be better understood and managed without throwing dinnerware across the room at ungrateful family members. And that’s the aim of this article: to arm you with factoids that you can hurl at those who yell at you for not taking better care of your diabetes.
Look at it this way: You might even be healthy enough to run for public office one day, or become a Supreme Court Justice, like Sonya Sotomayor, who’s also a T1D.
So, let’s dive into the four most important things about T1D that you should always remember.
#1 Diabetes is far more complex than you think
Many people see diabetes as a “complicated problem,” where, with enough learning and horsepower, it’s a knowable and repeatable process. All you need to do is come up with a formula—or an algorithm—and the disease is taken care of for you.
In reality, diabetes is “complex problem,” which is a type of problem where there are just too many variables, and each is too diverse and volatile to predict any outcome within any reasonable degree of certainty.
Therein lies the key idea: certainty and predictability. There are degrees, but the error bars are very wide.
You do the same thing every day, and yet, blood glucose swings happen seemingly in wild and unexplained ways: Insulin doesn’t absorb exactly the same every time, and food doesn’t absorb the way you expect. And those are only two (major) factors. But the long tail of other factors also weigh in, which is the topic of my article, Why Managing Glucose is so Tricky: More than just carbs and insulin are involved in the balance of blood glucose levels, as there’s a cacophony of hormones signaling around the body than that have an enormous effect on glucose levels.
Let’s start with a perspective that may be shockingly simple: The average person has between four and five liters of blood, so a “normal” blood glucose level of 100 mg/dL means that a typical person has about one teaspoon of sugar throughout their entire bloodstream. That’s a whopping 4.2g of glucose, which equates to about a teaspoon of table sugar. Here’s a visual representation:
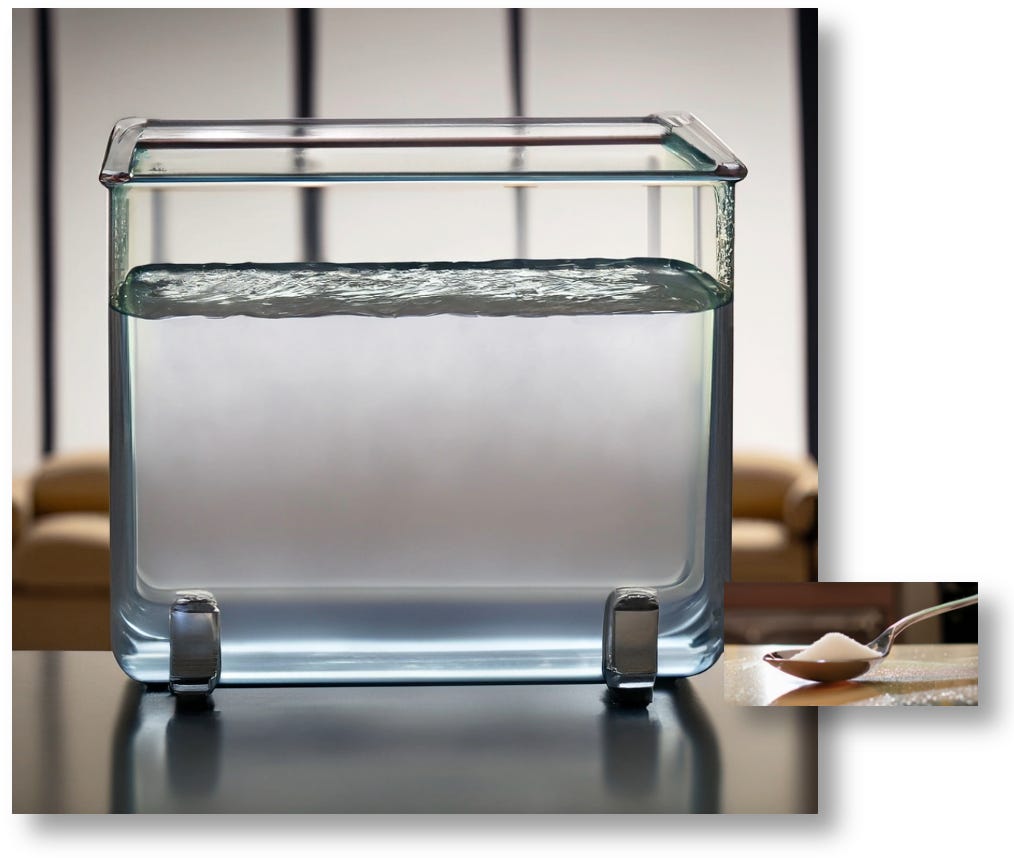
As you can see, 4.2g of glucose is proportionally tiny to the total volume of fluid. If you were to add 2.1g of glucose—a half a teaspoon of sugar—the total glucose content of this beaker would grow to 140 mg/dL.
But as any diabetic can affirm, eating a half teaspoon of sugar isn’t going to raise glucose levels to 140. So, where is all that glucose going?
That article goes on to explain that the body shuttles glucose around to different organs, often without the aid of insulin. What’s more, we also have hormones that cause the body to create glucose and deposit into our bloodstream (often, even if we don’t technically “need” it). This is an ongoing process, and incalculably complex.
The point is that the metabolic system is inherently volatile, even the natural human body has a very hard time keeping glucose levels stable. This is why there are 40 million type 2 diabetics in America, with another 98 million undiagnosed.
So, as a T1D, don’t necessarily buy into dogma that managing the disease can be reduced to singular things, like a specific diet, a behavior, or a technology. It’s all of them. And even then, they only work when you pay attention.
So if you have a hard time keeping glucose levels under control, you now know not to blame yourself.
But then you wonder, what the hell are my doctors telling me! After all, they’re the ones who give you prescriptions and tell you what to do, so how is it not their fault?
Let’s explore that.
#2 The impossible task of T1D docs (and they’re not all equal)
When you were diagnosed with T1D, there was probably a group of well-intentioned people that taught you the basics of insulin and carbohydrates, and how to work all the technologies that measures glucose levels and administers insulin. We’re then sent home with a stuffed animal and a huge, sugar-free lollipop.
After a few years of struggling with the disease, we get angry with our docs because we think they’re not doing enough, or not listening to us, or any number of complaints. Most T1Ds change doctors an average of 5-6 times during their first ten years, primarily for these reasons, only to run into the problem with each one.
The reality is that, even if a doctor could spend 100% of their time with you for weeks or months on end, there would be too many situations where it just isn’t clear which of a litany of possible explanations would explain why your glucose levels aren’t stable on any given day, night, or situation. Even endos that are also T1Ds don’t necessarily manage their own glucose levels very well either.
In a study that asked 17 physicians from 11 countries to provide insulin dose adjustments for 15 T1D patients, (based on charts showing glucose patterns) there was only a 51% agreement among the physicians. Among them all, there was a 17% change in just the basal rates.
So, what about automated insulin pumps? As it happens, that study also had an automated insulin pump algorithm, the Advisor Pro, perform similar analysis, and it too had great variability in recommendations that were not just different from the endos, but resulted in similarly erratic outcomes.
This all brings us back to the fact that diabetes is a highly complex disease—it has inherent volatility and unpredictability, even for non-diabetics—so you have to set realistic expectations, both of the disease, and of your care team.
Instead, use your empirical experiences to learn how your body works. Look for patterns and deal with them individually and independently. Think of yourself as a researcher, and you have a patient that receives 100% of your attention: YOU.
No one can hold your hand here. Figuring out your own unique T1D eccentricities is more art than science, and you can’t rely on clinicians or automated algorithms for this.
When I broached this topic with Christopher Worsham, a critical care physician and research faculty member at Mass General Hospital & Harvard (and co-author of "Random Acts of Medicine"), he told me:
“Not only are the disease and its treatment complex, but the way that complexity has to weave its way into the unique considerations for each individual patient with unique needs that change over their lifetimes makes it exponentially more complex. It's a situation where I think doctors/healthcare providers often need to take an approach of being an advisor to an informed and proactive patient, who is ultimately the one who is in control of their care (and will be the second they walk out of the office). That doesn't mean handing over the prescription pad, but it does mean having the humility to recognize when patients are, in fact, experts in their own disease and to help them take control of it in a way that the evidence suggests is going to be beneficial to them.”
The key phrase is, “an informed and proactive patient.” It takes considerable self-awareness to be proactive; you need to own your agency and just decide to make a commitment to it. Once you do that, becoming “informed” is a tad easier, but there are pitfalls. Namely, the desire to oversimplify, which leads to:
#3 Oversimplified explanations, oversimplified treatments
As mentioned before, many people treat T1D like a “complicated problem,” by reducing it into easy, bite-sized tasks that can be administered by patients. This is understandable, but it’s also a moral hazard, similar to problems that face politicians: Oversimplified information leads to oversimplified solutions. It may feel good to hear these ideas, but they often fail in real-world conditions. (Remember, I’m trying to talk about T1D here, not politics.)
The most universal example of this is insulin pumps. To be clear, there’s nothing wrong with pumps, per se. That is, by themselves, they are nothing more than an insulin delivery mechanism. The real problem is that people somehow believe that using pumps is somehow a simple, easy solution. And it isn’t.
The main problem with pumps is psychological: When they feel they are doing hard work that you don’t have to, you’re less engaged with T1D. It may feel wonderful to put T1D in the background of your day so you can lead a normal life, but it’s not that simple. While you’re not looking, the pump just has one goal: keep glucose levels lower. And to do that, they keep feeding increasingly larger doses of insulin.
While higher insulin rates lowers A1c levels, that only gives the illusion of progress. It also leads to a cascading series of unhealthy events, namely severe hypoglycemia and weight gain, both of which are highly unhealthy. Obesity in T1D has increased across the T1D community since 1988, when it was just 3.4%. Today, with the increased used of insulin pumps (where it’s extremely easy to administer insulin without much thought), the rate of obesity among T1Ds is now at 37% in 2023, according to the Lancet article, “Obesity in people living with type 1 diabetes.” Weight gain leads to cardiovascular disease, kidney and liver dysfunction, and a whole set of conditions normally only seen in T2Ds.
Having both T1D and T2D—a condition called “double diabetes”—is like a politician being both a Democrat and a Republican! That’s almost worse than a third-party candidate! (ba da boom!)
Sorry about that.
Ok, the problem is understandable, and even a bit poetic: The medical system wants to teach something… and yet, it can’t teach everything… but it’s better than nothing.
The same can be said of diets, supplements, and so many other things. The only way to achieve healthy outcomes is to stay engaged with your T1D.
To illustrate that, let’s move to factoid #4:
#4 Stay Engaged!
Leave it to technology entrepreneurs to make things easier, faster, and simpler for everyone. But not less expensive. (Remember that.) To quote H. L. Mencken: “For every complex problem, there is an answer that is clear, simple, and wrong.”
As noted above about the problem with insulin pumps—the psychological belief that it will do the work for you—disengages people from their disease.
We live in a time of rapid technology advancement, from AI to drugs to devices, and we’re told (and we believe) that these can make us healthier more easily.
In some respects, this is true. Consider the CGM (continuous glucose monitor): It is has had the most positive impact on T1D management for two key reasons: 1) It’s very easy and accessible, and 2) the patient has data available by looking at their phone, a habit that (sadly) is part of human life across the globe. All T1Ds that use CGMs have far superior health outcomes than those who don’t use CGMs solely because the devices encourage engagement.
Interestingly enough, this is also an advantage of insulin pens (or syringes). While many people hate the process of sticking themselves multiple times a day (hence the term, “MDI”—multiple daily injections), those who use pens are more likely to be engaged with their disease because they have to pay attention—not just by having to dose, but by thinking more carefully about how much to dose. And that often has an effect on people’s diets.
“How much insulin should I take for this glazed donut that I know I shouldn’t eat?”
Studies show that when people have to think about this, they may choose not to eat the donut far more frequently than pump users.
But of course, engagement requires a degree of maturity, not just cognitively, but physiologically. Your body has to have stabilized beyond the adolescent phase when hormonal activity is pretty volatile. This is why those over the age of 26 are far more engaged with their T1D than younger folks.
It’s this level of engagement that starts to blur the effectiveness of pumps vs. MDI, as illustrated by this study by the T1D exchange in 2018. See this chart from the study:

These results have been replicated along a series of studies covered in this metareview of randomized control trials using closed-loop systems, which showed that adult subjects only saw an improvement of only 1.07% compared to those not using pumps.
There’s another factor: Cost. In a paper titled, “Cost-effectiveness of Initiating an Insulin Pump in T1D Adults Using Continuous Glucose Monitoring Compared with Multiple Daily Insulin Injections: The DIAMOND Randomized Trial,” researchers found that the lifetime cost for pump users would be $112,045 more than MDI (multiple daily injections), along with a decrease in quality-of-life metrics by 0.71, and a decrease in life expectancy by 0.48 years.
The authors conclude, “initiating an insulin pump in adults with T1D already using CGM was associated with higher costs and reduced quality of life.” This is primarily why insurance companies are so resistant to covering insulin pumps in their policies.
This all points to why children and adolescents (as shown in the study) perform better with pumps: Because they have not yet developed that maturity. In essence, an automated pump will actually do something—even if non-optimal—but it’s better than someone that does nothing at all.
The real rub that causes the visceral arguments and dinnerware to be hurled across the room is that the medical community’s efforts to streamline care puts most T1Ds on pumps, without evaluating on a case-by-case basis whether it's appropriate for any given patient. Even the ADA guidelines instruct caregiver to evaluate the appropriateness of insulin pumps for patients on a case-by-case basis. But again, who has time for that?
For a much deeper dive into this, see my article, Benefits and Risks of Insulin Pumps and Closed-Loop Delivery Systems, which delves into the epidemiological research that surprises many.
What the article point out is that the most beneficial thing one can do is learn about T1D and your own unique physiology. In the literature review, “Diabetes Technology: Standards of Medical Care in Diabetes—2022,” the authors find that no technology has succeeded in reducing A1c levels below the 7% threshold in large populations. Only the user can do that by being engaged with their disease. This is their concluding statement:
“The most important component in all of these systems is the patient. [...] Simply having a device or application does not change outcomes unless the human being engages with it to create positive health benefits. [...] Expectations must be tempered by reality—we do not yet have technology that completely eliminates the self-care tasks necessary for treating diabetes.”
Summary
I once had an endocrinologist in the 1980s that was also a T1D, and I always asked him what his A1c was, but he never answered me, always giving me vague, sweeping answers, couched in the form of advice.
One day, as I was paying my bill with the receptionist, I commented to her that I assumed his T1D was in great control because, you know, he’s an endo! But she looked at me and rolled her eyes. Then she signaled to me to lean forward to tell me something.
She said his control was horrible because “he spends all his time in the office, eats poorly and doesn’t exercise.” She then added matter-of-factly while continuing her paperwork, “People who are in the best control just pay attention to their numbers, and do what they know they should do. It’s not magic. You just have to decide to do it.”
It felt as though this was the best kept secret in the whole world. Simple, yes. Inexpensive. No complicated technology. Nothing to promote, buy or sell. And yet, it would be another thirty years before I considered her observation, largely because I thought it would be hard, daunting, painful, and an abrupt imposition on my lifestyle. You know, “work.”
But, once I decided to do it in 2018, it became such a non-issue, I couldn’t believe I waited that long. Once I removed the word “work” from my vocabulary, it truly felt “easy.” I write about this in my article, The Four Habits of Healthy T1Ds.
For more inside info on how I managed to stay alive, see my article, Why I Haven’t Died Yet: My Fifty Years with Diabetes.
It may sound like managing T1D is difficult, but it’s much easier than solving our political problems.